Your digestive system is constantly communicating with you. A mild stomach ache after a heavy meal is normal. But some symptoms are your body’s urgent way of saying something is wrong. The challenge is knowing the difference.
In India, many patients wait months — sometimes years — before seeking specialist care for digestive symptoms. By then, what could have been treated simply has become complex. Here are 10 warning signs that should never be ignored.
Sign #1
Blood in Your Stool or Toilet Bowl
Bright red blood may suggest haemorrhoids or an anal fissure — usually not dangerous, but worth confirming. Dark, tarry stools, however, can indicate bleeding higher in the digestive tract and require urgent evaluation. Never assume blood in the stool is ‘normal’.
Sign #2
Unexplained Weight Loss
If you are losing weight without trying to — more than 4–5 kg over a few weeks — without changes in diet or activity, this warrants investigation. Unexplained weight loss is one of the early warning signs of gastrointestinal cancers.
Sign #3
Persistent Abdominal Pain
Occasional stomach discomfort is common. Pain that is severe, comes in waves, or has lasted more than 2–3 weeks is not. This can indicate conditions ranging from peptic ulcers to gallstones to more serious problems requiring surgical evaluation.
Sign #4
Difficulty Swallowing (Dysphagia)
Feeling food ‘stuck’ in your throat or chest is called dysphagia. If this is happening regularly, it may signal a narrowing of the oesophagus, acid damage, or in some cases, a tumour. It should never be dismissed.
Sign #5
Persistent Heartburn or Acid Reflux
Heartburn more than twice a week that does not respond to antacids is a sign of Gastro-Oesophageal Reflux Disease (GERD). Left untreated, chronic GERD can damage the lining of the oesophagus and increase cancer risk.
Sign #6
Sudden Change in Bowel Habits
A new pattern of diarrhoea or constipation lasting more than 4 weeks — especially if you are over 45 — should be evaluated. This includes changes in stool frequency, consistency, or shape (very thin stools can be significant).
Sign #7
Anaemia Without an Obvious Cause
Low haemoglobin (anaemia) that is not explained by diet or menstruation may signal slow internal bleeding in the gastrointestinal tract. This is a common presentation of bowel cancer in early stages.
Sign #8
Visible Abdominal Swelling or a Lump
A noticeable bulge in the abdomen, groin, or navel — especially one that appears when you cough or strain — may be a hernia. Other causes of abdominal swelling include fluid accumulation (ascites) or organ enlargement, all of which need assessment.
Sign #9
Nausea or Vomiting That Won’t Stop
Occasional nausea is harmless. Nausea or vomiting that persists for several days, recurs frequently, or is accompanied by pain, fever, or weight loss requires immediate attention. It may point to a blockage, infection, or gastroparesis.
Sign #10
Jaundice (Yellowing of Skin or Eyes)
Yellow skin or eyes, dark urine, and pale stools together suggest that bile is not flowing properly. This can indicate gallstones blocking the bile duct, hepatitis, or in more serious cases, pancreatic or liver conditions.
BOTTOM LINE: These signs do not always mean something serious — but only a specialist can tell you that for certain. An early consultation can give you clarity, peace of mind, and in many cases, a much simpler treatment path.
Don’t wait. Book a consultation today — Phone: 081465 87090 | www.drbedi-gastrosurgeon.com
Cirrhosis – cirrhosis due to any cause increases the risk of liver cancer
Diabetes – It can result in fatty liver disease and thus leading to hepatitis and predisposes to cancer.
Non alcoholic fatty liver disease – it can lead to inflammation of liver cell thus predisposing to formation of cancer.
Hereditary conditions like hemochromatosis( iron deposition in liver), Wilson disease ( copper deposition in liver)
Aflatoxins – consumption of food product infected with fungus producing aflatoxins can also produce liver cancer
How can liver cancer be prevented?
Prevention is very important when it comes to a disease like liver cancer. The underlying cause of liver cancer is often liver inflammation and the development of a condition called Cirrhosis. In addition to avoidance of drugs and alcohol, infection (such as Hepatitis B or C) and obesity can contribute to the development of liver cancer.
Steps to minimize these risks include
Vaccination against hepatitis B for those at risk,
Prompt treatment for patients infected with hepatitis C,
Maintaining a healthy weight through diet and exercise.
Avoidance of alcohol
Good control of diabetes.
How is liver cancer detected?
Patients diagnosed at an earlier stage have better outcomes. There are many strategies that are used to detect liver cancer, including.
Routine physical exams with blood testing in high risk patients.
Several researchers are looking to find the one blood test that will help identify liver cancer much sooner. Until that time, we continue to remain vigilant and screen with a variety of methods to try to catch this disease as early as possible.
Are fatty liver disease and liver cancer related?
Fatty liver disease progressing onto non-alcoholic fatty liver disease(NAFLD) and non-alcoholic steatohepatitis(NASH) can result in cirrhosis of the liver. Cirrhosis of the liver predisposes the patient to liver cancer. The fatty liver itself does not predispose a patient to cancer however if it is controlled at an early stage before it progresses onto cirrhosis then the risk of liver cancer is negligible.
What is the optimal treatment of liver cancers?
In general, the basic approach of any cancer therapy can also apply to liver cancer. The treatment of the local disease. In liver cancer, we often address the local disease with:
Surgery (removal of the tumor) – treatment of choice for patients without cirrhosis of the liver.
Liver transplantation – it is the treatment of choice in patients with cirrhosis provided tumor size and number criteria are met. It takes care of cirrhosis of the liver also.
Radiation therapy
Local ablation of the tumor by radiofrequency
Catheter-directed chemotherapy or embolization.
Are herbal medicines recommended to treat liver cancer?
The term ‘herbal medicine’ can represent thousands of compounds. Unfortunately, most are not rigorously tested or regulated by the companies that produce them, so real evidence of any benefit is not known. In fact, they may have harmful side effects that one comes to know only after using them.
Should I be worried if I have a cyst on my liver?
There is often nothing to worry about with simple cysts in the liver. They can be quite common. When we find cysts that are growing, we will often take extra care to ensure that
There is not an associated tumor causing the growth
That cyst is not causing problems.
This is often discussed over time with your hepatologist and/or liver surgeon who can help in differentiating malignant ( cancerous) cysts from nonmalignant ones.
What should I do if some lesion is found in the liver on a regular check-up?
Lesions in the liver on ultrasound can be of many types
Non-cancerous
Hemangioma ( abnormal formation of blood vessels)
Abscess ( pus collection in liver)
Granulomas in liver- because of TB , Sarcoidosis etc.
Cysts of liver – that can be simple cyst or hydatid cysts ( worm infestation)
Cancerous
Primary liver cancer
Metastatic tumor from some other organ- liver is most common site of spread of tumors from other abdominal organs.
Neuroendocrine tumor of liver
Malignant cysts of liver
A hepatologist or liver surgeon can help you in guiding you towards diagnosis and treatment by carrying out relevant investigations.
If a parent had/has liver cancer, are their children at greater risk of getting it?
In some cases, yes, a parent with liver cancer can raise your personal risk e.g in hereditary disease as Hemochromatosis, or Wilson’s disease. However, this is not true for the majority of patients. It’s always good to talk to your primary care doctor about your concerns or questions.
Gall bladder diseases are very common these days. These diseases range from innocuous gall stones to cancer of the gall bladder which has a very dismal prognosis. As a GASTROINTESTINAL SURGEON with HEPATOBILIARY experience we daily see cases from one extreme to another. The majority are simple gall stones and are managed at the periphery, however, what we receive are ones that are either left to be referred to as higher-level or are complicated ones. Many a times we also deal with cases that are operated elsewhere and become complicated and are then referred to us.
So today in this blog I would like to discuss gall bladder diseases with a special focus on stone diseases. The most commonly asked questions in the patient’s mind are
How are stones formed?
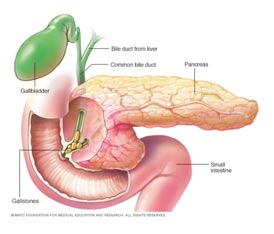
Bile is juice produced by the liver and stored in the gall bladder and released when food reaches the small intestine. It is composed of bile salts, and pigments, and they are kept in solution form by mixing with cholesterol. So any change that disturbs this proportion of each component required to keep these in solution form can result in the formation of stones. For example diet rich in fats can result in high cholesterol components and can result in stone formation.
How can we prevent formation of gall stones?
Gall stones are usually formed by a mismatch in the concentration of cholesterol and bile salts in bile. So a balanced diet that is low in fats can help in decreasing the chances of gall stone formation.
What are risks associated with gall stones?
Gall stones can cause pain by themselves. They can result in jaundice if a stone slips into bile duct. It can cause pancreatitis which can be mild or life-threatening. The gall bladder neck can be blocked by stone resulting in huge distension of the gall bladder thus causing pain and can result in pus formation in the gall bladder. Large stones in gall bladder are risk factors for cancer of gall bladder.
If they are not causing any trouble, should I undergo surgery?
These are called asymptomatic stones. Asymptomatic stones usually do not require surgery unless
a. Patient is having low immunity
b. The patient is living in a place where medical facilities are meager.
c. Patient is undergoing surgery of abdomen for some other reason Relative indications are
i. Multiple small stones
ii. Diabetic patient
iii. Large stone
Can we just remove stones and leave gall bladder behind?
We have to remove the gall bladder as its functionally abnormal and stones would reform. Moreover cut on gall bladder heal very poorly.
Will removal of the gall bladder affect my digestion?
There is no effect on digestion if the gall bladder is removed. Body adapts to removal of gall bladder very well and digestion is not affected at all.
What are dietary restrictions after gall bladder surgery?
There is no dietary restriction and the patient can have a normal diet as before. Digestive system adapts well to removal of gall bladder and there is no effect on the digestion of food.
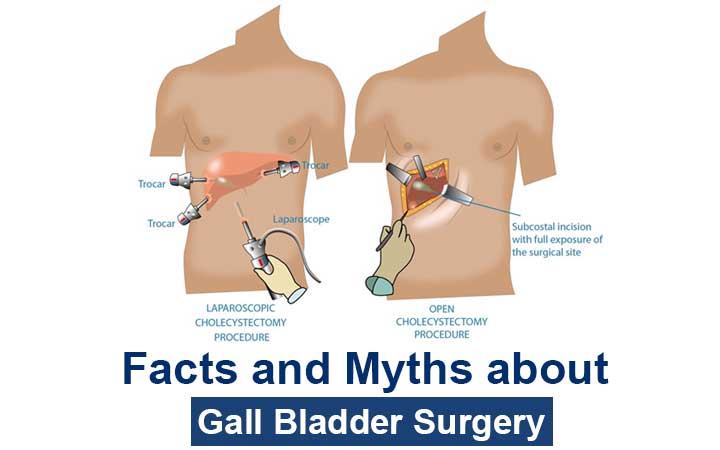
Is it major surgery?
Gall bladder removal surgery is performed by laparoscopy. It is successful in more than 99% of cases. Occasionally it is done by open surgery if anatomy is difficult or there is a risk of injury to important structures. But as the experience of the surgeon increases chances of conversion to open procedure decrease.
Is it very painful?
Laparoscopy surgery is done through small cuts made on your tummy ranging from 0.5-1 cm. these are small cuts and pain is minimum.
Should we undergo open or laparoscopic surgery?
That is to be decided by the surgeon operating upon you. As mentioned above large majority of procedures can be done by laparoscopy and needs open surgery only if surgery is difficult or in the presence of gall bladder cancer.
How long does it take to remove gall bladder?
Surgery is never about time. It is better to finish the procedure safely than quickly. It may take from 10 mintues to an hour depending upon anatomy.
What are the risks of surgery?
Apart from anaesthesia risk that depends upon general condition of patient gall bladder surgery carries minimum risk. Still there is a small but real risk of bleeding, injury to bile duct or injury to bowel.
How long does it take to recover and get back to normal life?
Gall bladder surgery is usually done as daycare surgery and the patient is send home same evening of surgery. The patient is up about a Few hours after surgery and starts his normal routine within a few days of surgery.
How does the experience of the surgeon matter in gall bladder surgery?
The experienced surgeon has fewer conversion rate and the chances of complication are less. Surgeon experienced in hepatobiliary or gastrointestinal surgery can handle the majority of complications on table and can provide better outcome in difficult cases.
Why some people are unsatisfied after gall bladder surgery?
Gallstones can cause abdominal pain, bloating, or discomfort after food intake and the complications listed above. Symptoms such as indigestion, heartburn, constipation and increased frequency of stools are very common in the general population and are not related to gallstones. Mostly when the patients / treating doctors try to correlate these symptoms with gallstones it leads to unhappiness as these symptoms may not get relieved by the removal of the gall bladder. So proper patient selection and counseling can help avoid the unsatisfied patient.
Known causative factors for gall bladder cancer are
Gall Stones
Gall bladder Polyps
Porclein gall bladder
Obesity
Old age
Choledochal cyst
Abnormalities of union of bile and pancreatic duct
Primary sclerosing cholangitis
Ethnicity
People residing in high-risk area eg., Chile, along plains of river Ganges etc.
2. What are signs and symptoms of gall bladder cancer?
Gall bladder cancer can present with very non-specific signs and symptoms. Majority times it is detected incidentally on imaging. Patient may present with
Pain
Jaundice
Loss of weight
Loss of appetite
Distension of abdomen
3. How can gall bladder cancer be detected?
Gall bladder cancer usually are detected on imaging. Ultrasound abdomen is first lie of investigation that can show irregular thickening of gall baldder wall. These findings are confirmed by multiphasic CECT abdomen that can show condition of gall bladder and surrounding enlarged lymph nodes.
4. Are gall bladder polyps cancerous?
Small gall bladder polyps are non cancerous. Any polyp larger than 1 cm in size harbour higher chances of malignancy and is an indication of surgery.
5. How can gall bladder cancer be prevented?
Gall bladder cancer cannot be prevented . There are no ways by which gallbladder
cancer can be prevented except for prophylactic cholecystectomy in area of high endemicity eg., Chile , where prophylactic cholecystectomy had been shown to decrease incident of gall bladder cancer.
6. What is treatment of gall bladder cancer?
Main treatment of gall bladder cancer is surgery is it is feasible. Complete resection of gall bladder cancer is the only chance of providing long term survival. Usually majority of patients present with advanced disease that cannot be resected and can be offered palliative treatment only. Resectability if usually assessed best by liver/gastrointestinal surgeon who is experienced in liver surgery. Assessment by liver surgeon can make advanced disease resectable by proper planning with help of interventional radiologist. Chemotherapy has a role in pallative setting or after resection of tumor by surgery.
A colon, also called the large intestine or large bowel, is part of the body’s digestive system. The colon is a muscular tube about five feet long and three inches wide. During digestion, food moves from the stomach to the small intestine and then to the colon. The colon absorbs water and nutrients from the body’s waste, creates stool and then pushes that stool into the rectum.
2. What is the differences between colorectal, colon and rectal cancer?
Colorectal cancer is the term used to describe cancer of the colon and/or rectum. The two cancers are grouped together because they share many common characteristics. Together, the colon and rectum make up the large intestine, a question mark-shaped bowel four feet in length. Colon cancer develops in all but the last few inches of the large intestine, between the appendix and rectum. Rectal cancer develops in the rectum, the last few inches of the large intestine that attaches to the anus. Colon cancer is more common.
3. What are polyps?
A polyp is a clump of cells that forms on the lining of the colon giving rise to swelling that project from wall of colon into lumen of colon. Most polyps are not harmful, but some may develop into colon cancer. Colonoscopies can help detect pre-cancerous polyps
4. What are sign and symptoms of colon cancer?
Colorectal cancer may develop when benign polyps in the large intestine grow and become cancerous. If early-stage colorectal cancer does cause symptoms, early warning signs may include sudden weight loss and/or narrow, ribbon-like stools. Other common early warning signs of colorectal cancer include:
Rectal bleeding, either bright or dark red in color
Tenesmus, which is the feeling that you have to empty your bowel but nothing passes
Anemia caused by iron deficiency
Persistent abdominal pain
As the cancer grows, symptoms may include:
Abdominal pain or cramps
Constipation
Diarrhea
Blood in your stool
Bloating or a sense of not feeling empty after a bowel movement
Flat or ribbon-shaped stool
Unexplained weight loss
Fatigue
Loss of appetite
5. What are risk factors for colon cancer?
A risk factor is something that increases your chances of getting a disease. Having a risk factor does not mean that you will definitely get a disease, only that you and your doctor should watch more carefully for warning signs. Some risk factors can be avoided through lifestyle changes and some cannot. Some of the risk factors for colon cancer include:
Age 50 or older
Type-II diabetes
Personal or family history of colon cancer or polyps
Personal history of inflammatory bowel disease
Some inherited genetic syndromes
Diet high in fat and/or low in fiber or calcium
Obesity
Smoking
Heavy drinking
Physical inactivity
6. How is colon cancer diagnosed?
Doctors use many tools and techniques to diagnose colon cancer including:
History and physical examination by a physician
Testing blood and stool
Performing colonoscopies
Performing CT scans, PET scans, MRIs, endoscopies, and ultrasounds
7. How can we prevent / decrease risk of colon cancer?
The risk factors for colorectal cancer may be reduced with regular checkups and lifestyle changes. In western countries it is recommended that men and women have a colonoscopy beginning at age 50 as the rates of cancer are higher in west. If you have a family history of colorectal cancer, you should get screened 10 years earlier than when your family member was diagnosed. For example, if your father was diagnosed with colon cancer at 48, you should talk to your doctor about getting a colonoscopy at 38. Talk to your doctor about how often you should get a colonoscopy. The procedure may be able to help your doctor spot cancer in its early stages. Pre-cancerous polyps are removed and biopsies are performed during the procedure, if necessary.
Changes in your lifestyle may also help you lower your risk and prevent colorectal cancer from developing. Obesity, smoking, alcohol, diet and a sedentary lifestyle have been linked to an increased risk for colorectal cancer
8. Is colon cancer hereditary?
Colorectal cancer isnt always passed down in families, but it can be. If someone in your family has had colorectal cancer, you may be more likely to develop it.
Colorectal cancer can sometimes be caused by Lynch syndrome, a genetic condition also called hereditary nonpolyposis colorectal cancer (HNPCC). About one in 30 colorectal cancer cases are a result of Lynch syndrome. Patients with Lynch syndrome tend to get colorectal cancer at a younger age than others, with a higher likelihood of developing other types of cancer as well, such as:
Stomach cancer
Liver Cancer
Ovarian Cancer
Uterine Cancer
9. How is colon cancer treated?
Surgery is the most common form of treatment for colorectal cancer. Surgery is used to remove the tumor and surrounding tissue. A portion of the colon or rectum may need to be removed, and a colostomy( part of colon is brought out through abdominal wall and bag if fixed over it in which stool gets collected) may be required—permanently or temporarily, depending on the extent of the cancer and how much of the colon or rectum is removed. Other treatment options include chemotherapy and/or targeted therapy drugs, which may also be used in addition to surgery. Radiation therapy is usually an option only for rectal cancer, not colon cancer.
10. What types of doctors will I see during my treatment?
Your colorectal cancer care team may include one or more of these doctors:
A gastroenterologist, who specializes in the digestive system and performs colonoscopies
Surgical gastroenterologist/ GastroIntestinal Surgeon – who performs surgery to remove tumors and provide best functional outcome e.g pouch formation in case of hereditary cancers. If disease is early only surgery can be curative.
A radiation oncologist, who uses radiation therapy to treat cancer
A medical oncologist, who treats cancer with drug therapies.
Surgery is the mainstay of treatment in colon cancer. Preoperative chemoradiation is used in rectal cancer in locally advanced cases. Surgeon can assess the local stage of disease on scans and thus can plan upfront surgery or chemoradiation. Postoperative chemotherapy/radiation therapy is decided after final stage of disease is determined after examining removed specimen.
Robot-assisted surgery is a type of minimally-invasive surgery completed through small incisions. The da Vinci surgical system uses high-definition, three-dimensional cameras that magnifies image 20 times coupled with specialized surgical tools that enable surgeons to operate with more precision and better control.
The robotic instruments have mechanical wrists that bend and rotate to mimic the movements of the human wrist thus allowing surgeons to make precise movements. Robotic software also negates the effect of surgeons’ hand tremors.
It is an effective minimally invasive alternative to both open surgery and laparoscopy. Surgeons undergo vigorous training with this system before being allowed to use it for surgery on patients. Moreover, there are many inbuilt safety checks in the system that decreases the chances of error. Patients can be rest assured knowing they’ll receive superior surgical care for the best possible outcome.
How robot-assisted surgery works ?
During robotic surgery, your surgeon inserts a tiny camera through a small incision in the surgical area. The camera sends a high-definition, 20 times magnified, 3D image of the surgical site to an external monitor in real-time.
Using computer-assisted technology that guides specialized surgical instruments, your surgeon directs the robot with better control, precision, and range of motion than is possible with traditional surgery. A support team assists the surgeon with other surgical tasks. Thus the use of a robotic system makes difficult steps easier for the surgeon by providing a range of motion and more maneuverability in handling tissue and suturing.
Will the surgeon be with me in the operating room?
Many patients wonder who is operating on them: the robot or the surgeon.
Robot-assisted surgery is a system that enables surgeons to operate with precise, delicate motions by controlling the machine. The robot never makes decisions or performs incisions on its own — it only responds to your surgeon’s hand and finger movements.
Your surgeon is located at a console in the operating room near you and the experienced support staff, directing the procedure the entire time. The robot allows for greater precision than the human hand has on its own, and your surgeon is in charge the whole time.
Conditions that can be treated with robot-assisted surgery
The majority of gastrointestinal issues can be addressed using robotic-assisted minimally invasive surgery, including:
Appendicitis
Hernias
Gallbladder disease and its cancer surgery
Gastroesophageal reflux disease (GERD)
Liver surgery
Surgery of the pancreas including surgery for cancer of the pancreas
Surgery for the colon and rectum including its cancers
Surgery for the esophagus, stomach, and intestine
Gastrointestinal and liver cancer surgery.
The benefits of robotic surgery
Robot-assisted surgery has many benefits. Patients experience these benefits both directly and indirectly. For example, because robot-assisted surgery is minimally invasive, a direct benefit to you is a shorter recovery time. And because the surgeon has better access to the operative area, an indirect benefit is a more precise surgery.
Other benefits include:
Smaller incisions
Greater range of motion and dexterity for the surgeon
High-resolution, the highly-magnified image of the operating field for better visualization during surgery
Shorter hospital stay
Lower risk of infection
Reduced risk of blood loss
Faster recovery with less pain
Minimal scarring
Better clinical outcomes
In addition, due to the enhanced control, flexibility, and precision that robot-assisted surgery offers, surgeons can complete complex or delicate procedures that may be difficult or impossible with traditional surgery.
Am I a candidate for robot-assisted surgery?
Although robotic surgery offers excellent outcomes for many patients, not everyone is a good candidate. The patient is recommended against robot-assisted surgery if:
You’re unable to have general anesthesia
You have significant scar tissue or other issues that prevent the cameras from visualizing the surgical area
You’ve been diagnosed with bleeding problems that put you at risk for surgery
You’re not a candidate for laparoscopic surgery
After a full evaluation of your condition and overall health, the surgical team in charge will determine if robot-assisted surgery is right for you.
What Are the Advantages of Robotic Surgery Over Laparoscopic Surgery
Robotic surgery is a minimally invasive surgical technique that uses a robotic arm to perform surgery.
The robotic arm is controlled by the surgeon, who sits at a console and uses a joystick to manipulate the arm. This allows the surgeon to perform surgery with greater precision and dexterity than is possible with laparoscopic surgery.
If you are considering robotic surgery, here are some things you can expect:
You will be given general anesthesia, which will put you to sleep during the surgery.
The surgeon will make a small incision in your abdomen and insert the robotic arm.
The surgeon will then use the robotic arm to perform the surgery.
The surgery will typically take less time than traditional open surgery.
You will likely be able to go home the same day or the next day after the surgery.
Overall, robotic surgery is a minimally invasive surgical technique that offers several advantages over laparoscopic surgery. If you are considering surgery, talk to your doctor about whether robotic surgery is a good option for you.
Advantages of Robotic Surgery
Here are some of the specific advantages of robotic surgery over laparoscopic surgery:
Improved visualization: Robotic surgery provides the surgeon with a magnified, 3D view of the surgical site. This allows the surgeon to see more clearly and make more precise movements.
Greater dexterity: The robotic arm has a greater range of motion than the human hand. This allows the surgeon to reach areas that would be difficult or impossible to access with laparoscopic surgery.
Tremor-free movements: The robotic arm is tremor-free. This means that the surgeon can make very precise movements without the risk of shaking.
As a result of these advantages, robotic surgery has been shown to have several benefits over laparoscopic surgery, including:
Less pain: Robotic surgery is associated with less pain and a shorter recovery time.
Lower risk of complications: Robotic surgery is associated with a lower risk of complications.
Better cosmetic outcome: Robotic surgery is associated with a better cosmetic outcome.
However, it is important to note that robotic surgery is not always the best option for every patient. Some patients may be better suited for laparoscopic surgery or traditional open surgery. It is important to discuss your options with your doctor to determine which type of surgery is right for you.
Constipation is a common problem affecting people of all age groups. It has many definitions according to people understanding and myths. It is correlated with many symptoms and afflictions. Many problems are attributed to constipation and many homemade remedies are used to get over these problems. Basically we lack understanding of process of passing motion and thus have many wrong notions and myths about passing motion.
“There is no standard when it comes to passing motion. Everyone’s system is different, so if you’re concerned about how many times a day you should pass motion, it really depends on your body. Some people pass motion three to four times per day, others pass it once a week – and they’re fine, not sick. Everything from motion’s consistency (soft or hard) and fecal size, to how long it takes the body to pass feces( stools) is based on the individual. At what time one should pass motion is different for different individual and depends upon his food consumption previous day. What’s important is to your track any changes in bowel habits.”
When is time to consult your healthcare provider is when you notice the following changes in bowel habits:
Uncomfortable bloating
Pain while passing stools
Extremely hard stools, difficult to push out, or thin stools
Uncontrolled passage of stools, accidents in pants or bed
Feeling the colon never completely empties
Pooping, or lack thereof, disrupts day-to-day work and functionality
Passing Gas
It’d be hard to talk about passing of motion without mentioning passage of gas, or as some people call it, farting. Like passing stools, gas is related to bacteria in our digestive system, as well as the foods we eat.
“Gas is a by-product of bacteria in our large intestine digesting leftovers of the foods we ate. Bacteria produce hydrogen, nitrogen, oxygen, carbon dioxide and methane. Yes, it’s the methane that explodes, if you fart near a flame. There is no healthy or unhealthy amount of gas. How much gas you pass and the odor largely depends upon what you have eaten.
Foods that Make You pass stools easily
It’s no surprise that what we eat determines how we pass motion, more or less. Eating foods high in fiber is well known for helping ease time spent on the toilet and producing voluminous, bulky stools, sometimes gas, too.
“Fiber, both soluble and insoluble, holds moisture, keeping stools soft and bulky, which allows the colon to gently squeeze your stools through, as opposed to squeezing and straining to pass small hard bowel movements, possibly with cramping and discomfort.
In addition to what you eat, how much you drink can also play a role.“Staying well-hydrated is important. You know you are well-hydrated if you’re urinating every three to five hours, and the urine is barely yellow. Generally, stools stays softer then, too.
You can try these natural laxatives to ease passage of stools for occasional use:
Apple juice
Coconut milk/juice
Aloe vera juice
Coffee
Tea
Fiber supplements
When is constipation a problem ?
A sudden and recent change in the routine of passing stools
Change in color of stool – black color
Change in consistency and shape of feces
Blood in stool
Loss of weight and appetite along with any of the above symptoms
Don’t be scared or shy in discussing these problems with your physicians as they may indicate development of tumor. These symptoms are more important in patients with family history of cancer. They should not cause worry as they are signs for early check up to catch disease at early stage.
The pancreas is a long, flat gland that sits tucked behind the stomach in the upper abdomen. The pancreas produces enzymes that help digestion and hormones that help regulate the way your body processes sugar (glucose).
What is acute pancreatitis?
Acute pancreatitis is an inflammation of the pancreas that occurs suddenly. It differs from chronic pancreatitis in that there is a discrete episode.
Acute pancreatitis which may be classified as mild, moderate or severe, depending on the amount of damage and organ dysfunction caused by the pancreatitis.
What are causes or risk factor of acute pancreatitis?
Causes of acute pancreatitis are :
Biliary stones are the cause of 35 to 50 percent of the cases of acute pancreatitis.
Alcohol intake is the second leading cause of acute pancreatitis.
Several drugs may cause pancreatitis e.g, immunosuppressants, estrogens, acetaminophen, sulindac. tetracycline, salicylates, erythromycin, pentamidine, thiazide diuretics, furosemide and valproic acid.
Viral causes include hepatitis A, B, and non-A/non-B; cytomegalovirus; mumps; and coxsackievirus.
Bacterial causes may include Legionella, mycoplasma and mycobacterium tuberculosis.
Parasitic infections may also cause acute pancreatitis.
Pancreas divisum (a congenital defect of the pancreatic ducts).
Metabolic imbalances (hyperlipidemia and hypercalcemia).
Sphincter of Oddi dysfunction.
Scorpion stings.
Trauma to pancreas may also cause acute pancreatitis.
What are symptoms of acute pancreatitis?
Upper abdominal pain is main symptom. Usually it is severe and radiates to back.
Nausea and vomiting are the other most frequent symptoms of acute pancreatitis.
Fever
High pulse rate.
Few patients may have jaundice.
Patient may have low blood pressure and confusion or coma may occur.
Can acute pancreatitis become chronic pancreatitis?
Yes. Chronic pancreatitis results when inflammation in the pancreas has caused damage and resulted in fibrosis, calcifications and ductal inflammation. It is also possible for patients with chronic pancreatitis to have episodes of acute pancreatitis. Chronic pancreatitis is slow self propagating disease that results in slow destruction of pancreas.
How is acute pancreatitis diagnosed?
Diagnosis of acute pancreatitis is usually made clinically when patient presents with typical pain of pancreatic origin that is pain upper abdomen radiating to back. Further tests helps in confirming diagnosis e.g,
Avoidance of known causes of pancreatitis (i.e., alcohol consumption) may help prevent the onset of the disease. Lifestyle factors such as obesity, alcoholism, hepatitis and others that contribute to a poor state of overall health lead to complications of acute pancreatitis and to a poorer prognosis for recovery.
What is treatment of acute pancreatitis?
The treatment of acute pancreatitis depends on its severity.
If the disease is considered mild, the patient is usually treated supportively with intravenous fluids, pain control medication, keeping close watch on patient’s general condition so that it does not deteriorates.
Severe pancreatitis requires close monitoring of the patient to detect possible systemic complications. The patient may be admitted to an intensive care unit. Organisms may reach the pancreas and infect it by crossing the colonic wall. Antibiotics may be used to prevent sepsis. These patients may have some organ failure thus require support for these failed systems.
Surgical debridement and drainage may be necessary if infected pancreatic necrosis (cell death) arises. CT scan-guided aspiration of necrotic areas may be done to identify the infecting organism so that it may be treated effectively. Surgical intervention is usually done 4 weeks after onset of pancreatitis.
Therapeutic endoscopic retrograde cholangiopancreatography (ERCP) may be performed in the early stages of acute pancreatitis to remove gallstones and may require sphincterotomy (cutting the sphincter muscle to allow drainage from the biliary/pancreatic tract).
What are possible complications of acute pancreatitis?
Complications can be localized or systemic.
Systemic complications are usually seen in severe acute pancreatitis. These include
Low blood pressure
Lung failure
Kidney failure
Inflammation may extend to surrounding organs such as the colon and stomach, gastrointestinal bleeding.
Localized complications include
Fluid collections
Pancreatic pseudocysts
Pancreatic necrosis
Pancreatic abscess
Is there hereditary link with acute pancreatitis?
No. There may, however, be genetic influence in chronic pancreatitis.
Liver cancer is increasing day by day. Its probably due to increase in incidence of cirrhosis of liver that predisposes to liver cancer. Causes of cirrhosis of liver –
1. Alcohol 2. Viral hepatitis’ 3. NASH – Non Alcoholic Steatohepatitis 4. Toxins 5. Autoimmune conditions- PBC, Autoimmune Hepatitis etc.
Above are main conditions that cause cirrhosis and predisposes to liver cancer. As the rate of obesity and Diabetes Mellitus is increasing all over world so is the rate of fatty liver and steatohepatitis (injury to liver) that predisposes to cirrhosis and thus liver cancer. So it becomes imperative for allpatients having above mentioned factors to be utmost careful in monitoring the progression of theirdisease to detect cancer at early stage.
FAQs
1. How can liver cancer be prevented?
Liver cancers can be prevented by keeping high risk patients under regular follow with tumor markers and ultrasound examination. Patient at high risk of getting liver cancers are mentioned above. So patients with above risk factors who have not progressed to cirrhosis should be treated according to cause e.g; stopping alcohol, decreasing weight, good control of diabetes, treating viral hepatitis etc.
2. What is peculiar about liver cancer and its treatment?
Liver cancers usually arise in patients with cirrhosis. This presents peculiar problem as these patients have damaged liver in addition to tumor. Damaged liver further shrinks treatment options for such patients. Moreover majority of these patients are unfit for any form of treatment due to damaged liver. So treatment is tailored according to status of liver disease and tumour size and location.
3. Is there any medical treatment of liver cancer?
Mainstay of treatment is surgery. Medical treatment is offered to only those cases that cannot be offered any surgery
4. How can liver cancers be treated?
Best way to treat liver cancer is by surgery. Surgery can be
Resecting tumor or tumor bearing liver
Liver transplantation
First option is feasible only in normal livers or in cirrhotic with small tumours. In patients with cirrhosis best treatment option is liver transplant provided tumor load is within one specific range. Liver transplantation takes care of diseased liver and tumor simultaneously and thus provides best chances of prolonged life.
In cases of tumor deemed unresectable or patient is unfit for transplant, interventional radiology provides solution for tumor treatment by
A. Radiofrequency ablation that has same results as surgery in cirrhotics, B. Tumor chemoembolization C. Internal tumor radiation by TARE
5. Which specialist is best to treat liver cancer?
Before starting any treatment liver or liver transplant surgeon must be contacted. Liver surgeon is best person to evaluate patients fitness and tumour resectability and can provide tailored approach that is best suited for patient’s condition as mentioned above.
 Book An Appointment
Book An Appointment